This overview includes information to help you prepare for the National Clinical Mental Health Counseling Examination. You will find details about the current case-study format, content areas, the July 2027 exam update, registration, scoring, retakes, and study resources.
Case Studies
11 in the current exam
Questions
130–150 total; 100 scored
Exam Time
225 minutes
Delivery
Pearson VUE test center or OnVUE
Exam Background and Purpose
The National Clinical Mental Health Counseling Examination, commonly called the NCMHCE, is developed by the National Board for Certified Counselors.
The exam measures whether an entry-level clinical mental health counselor can apply and evaluate counseling knowledge in realistic clinical situations.
The NCMHCE may be used as part of a state counseling-licensure process. It may also be used to satisfy an examination requirement for certain national counseling certifications.
Unlike an exam based mainly on isolated definitions, the NCMHCE presents client case studies that develop over multiple counseling sessions. Candidates must use the information provided to make appropriate clinical decisions.
Passing the NCMHCE does not automatically issue a counseling license or certification. Candidates must also satisfy the education, supervision, experience, application, and other requirements established by the applicable licensing board or credentialing program.
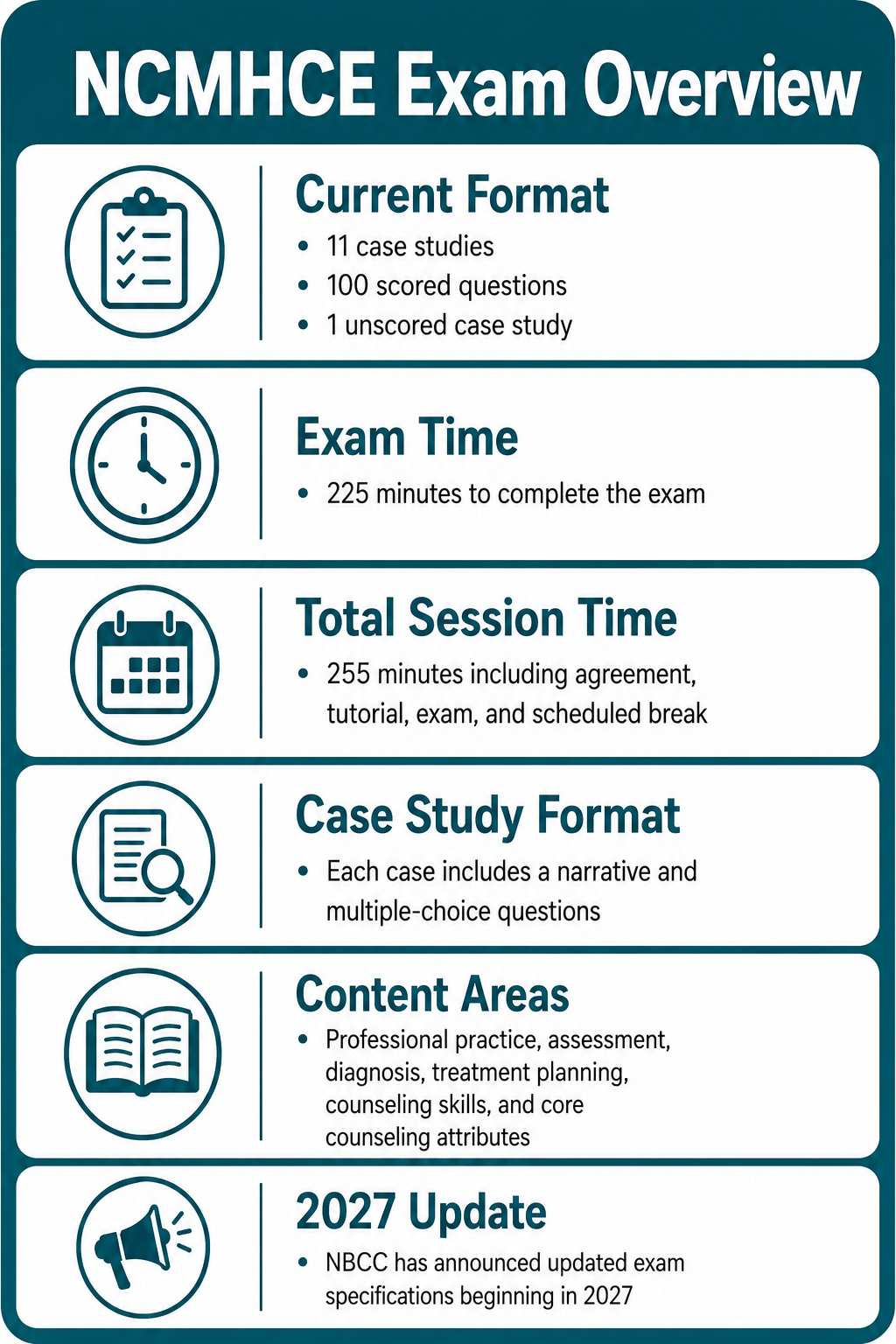
Current NCMHCE Format
The current examination format remains in effect through June 30, 2027.
It contains 11 clinical case studies. Ten case studies contribute scored questions, while one case study is unscored and is used to evaluate questions for possible use on future examinations.
Case Studies
- 11 total case studies
- One unscored case study
- 9–15 questions per case study
- Four answer options per question
Questions and Scoring
- 130–150 total questions
- 100 scored questions
- Remaining questions are unscored
- No penalty for an incorrect answer
Current Test Session
- Test Administration and Confidentiality Agreement — 5 minutes
- Testing tutorial and sample case study — 10 minutes
- Examination time — 225 minutes
- Scheduled break after the fifth case study — 15 minutes
- Total test session — 255 minutes, or 4 hours and 15 minutes
How Are the Case Studies Organized?
Each case study follows the development of a clinical relationship and is divided into three sections:
Initial Intake
Introduces the client, presenting concerns, history, symptoms, relationships, cultural context, and other available information.
Counseling Session One
Adds clinical information and may require assessment, diagnostic, ethical, treatment-planning, or intervention decisions.
Counseling Session Two
Continues the case and may address progress, new information, treatment revision, crisis response, referral, or termination.
Review all answers before leaving a section. Once you advance to the next section of a case study, you cannot return to or change answers from the previous section.
Current NCMHCE Content Areas
The current exam is based on six content domains. Five domains receive specific percentages of the scored questions. Areas of Clinical Focus is reflected through the diagnoses and presenting concerns used throughout the case studies rather than through a separate percentage of questions.
Professional Practice and Ethics
15% of scored questions
Informed consent, confidentiality, documentation, client rights, professional roles, counselor competency, supervision, referrals, social media, electronic communication, legal responsibilities, research concepts, and ethical clinical practice.
Intake, Assessment, and Diagnosis
25% of scored questions
Biopsychosocial interviews, diagnostic interviews, cultural formulation, mental status examinations, trauma and substance-use screening, risk assessment, assessment instruments, differential diagnosis, co-occurring conditions, and level-of-care decisions.
Areas of Clinical Focus
Evaluated throughout the case studies
Common presenting concerns may include anxiety, depression, trauma, grief, substance use, relationship issues, family concerns, suicidality, adjustment difficulties, identity concerns, behavioral concerns, and other clinical problems.
Treatment Planning
15% of scored questions
Client-centered goals and objectives, barriers to progress, intervention selection, consultation, referrals, coordination with other providers, treatment-plan revision, discharge planning, follow-up, and continuity of care.
Counseling Skills and Interventions
30% of scored questions
Counseling theories, therapeutic alliance, intervention selection, crisis intervention, psychoeducation, motivational strategies, family and couples counseling, group counseling, cultural responsiveness, client feedback, and management of the counseling process.
Core Counseling Attributes
15% of scored questions
Empathy, genuineness, congruence, positive regard, nonjudgmental practice, counselor self-awareness, conflict tolerance, sensitivity to multicultural and gender-related concerns, respect for diversity, listening, attending, and reflection.
Intake, Assessment, and Diagnosis plus Counseling Skills and Interventions account for 55% of the current scored questions.
Important July 2027 Exam Update
Updated NCMHCE specifications take effect July 1, 2027.
Candidates testing on or after that date should use preparation materials aligned with the revised exam domains and scoring system.
2027 Format
Case Studies
10 case studies
Questions
130–150 total questions
Field-Test Items
30–50 unscored questions
Exam Time
225 minutes
The 2027 exam will provide an optional 15-minute break halfway through the examination. Candidates will be able to review questions before submitting the first half, but they will not be able to return to those questions after beginning the break.
2027 Content Domains
Professional Development and Counselor Self-Awareness
15% of the exam
Continuing education, consultation, supervision, advocacy, competency, boundaries, self-reflection, self-care, vicarious trauma, burnout, countertransference, and professional limitations.
Intake and Assessment
18% of the exam
Informed consent, clinical interviews, biopsychosocial assessments, mental status examinations, risk assessment, trauma, substance use, diagnosis, assessment instruments, cultural considerations, and level-of-care decisions.
Treatment Planning and Continuity of Care
15% of the exam
Case conceptualization, SMART goals, treatment selection, culturally responsive planning, referrals, aftercare, relapse prevention, discharge, service disruption, progress evaluation, and termination.
Provision of Counseling Interventions
20% of the exam
Evidence-supported interventions, counseling theories, therapeutic alliance, crisis intervention, psychoeducation, group and family counseling, client feedback, cultural responsiveness, session management, communication, and therapeutic-rupture repair.
Indirect Client Care
12% of the exam
Collaboration with support systems, care coordination, interdisciplinary treatment, referrals, translation services, medication-effect documentation, clinical records, case notes, electronic records, and client advocacy.
Legal and Ethical Compliance
20% of the exam
State and federal law, ethical codes, mandated reporting, confidentiality, informed consent, record retention, telemental health, billing, reimbursement, emergency procedures, technology, artificial intelligence, licensure requirements, and professional liability.
2027 Scoring
Beginning July 1, 2027, NCMHCE scores will be reported on a scale from 100 to 500. A scaled score of 360 or higher will represent a passing result.
The scaled score will not represent a percentage. For example, a score of 400 will not mean that the candidate answered 80% of the questions correctly.
Eligibility and Registration
Registration requirements depend on why you are taking the NCMHCE.
State Licensure
Follow the eligibility, approval, registration, and score-reporting instructions established by the state counseling-licensure board.
National Certification
Follow the examination and application instructions associated with the applicable NBCC certification pathway.
Candidates normally register through the Credentialing Gateway. After registration and approval, Pearson VUE sends an Authorization to Test email containing the candidate ID and testing-window dates.
Registration Process
- Review the requirements for your licensing or certification pathway.
- Create or access your Credentialing Gateway account.
- Complete the required examination registration.
- Submit the applicable examination fee.
- Wait for the Authorization to Test email.
- Schedule through Pearson VUE after receiving authorization.
- Select a Pearson VUE test center or OnVUE when the desired option is available.
- Review the confirmation, identification requirements, and testing rules.
Costs and Payment
NCMHCE fees depend on the licensing, certification, military, or other credentialing pathway through which the candidate registers.
Additional expenses may include:
- State licensing-board application fees
- Credentialing application fees
- Transcript or education-review fees
- Background checks or fingerprinting
- Testing-window extensions
- Appointment-change charges
- Retesting fees
- Official score-verification requests
Confirm the complete cost displayed during registration before submitting payment. Examination fees are generally nonrefundable and nontransferable.
Testing Locations and Delivery Options
Pearson VUE administers the NCMHCE through two delivery methods.
Pearson VUE Test Center
- Computer and testing space are provided.
- Testing-center staff complete check-in.
- Personal items must be stored as directed.
- Unscheduled breaks do not stop the exam clock.
OnVUE Online Proctoring
- A compatible computer is required.
- A webcam, microphone, and reliable internet connection are required.
- The room and desk must satisfy security requirements.
- Unscheduled breaks are not permitted during the current online exam.
Only limited accommodations may be available through OnVUE. Candidates requiring testing accommodations should obtain approval before scheduling and verify which delivery option supports the approved accommodation.
What Should I Expect on Test Day?
Test-Day Checklist
- Confirm the appointment date, time, and delivery method.
- Complete the OnVUE system test before an online appointment.
- Arrive or begin online check-in at the required time.
- Bring acceptable government-issued identification.
- Make sure the identification name matches the registration record.
- Store or remove phones, watches, books, notes, bags, and unauthorized materials.
- Complete the confidentiality agreement and tutorial.
- Review every response before leaving a case-study section.
- Use the scheduled break according to the testing instructions.
- Answer every question because incorrect answers do not create an additional penalty.
How Is the Current NCMHCE Scored?
The current examination reports a pass-or-fail result.
Of the 130–150 questions, 100 are scored. Each scored question contributes one raw score point.
The minimum passing score is established through a professional standard-setting process. Statistical equating is then used to account for small differences in difficulty among examination forms.
Because of this process, the raw number of correct answers required to pass may vary slightly between forms.
The current exam does not use one fixed national percentage that candidates can calculate before testing.
Retaking the NCMHCE
Candidates who do not pass may register for another attempt.
- Wait at least 30 days before retaking the examination.
- Follow a longer waiting period when required by the applicable state licensing board.
- Complete a separate examination registration.
- Pay the applicable examination fee again.
- Obtain another Authorization to Test.
- Schedule a new Pearson VUE or OnVUE appointment within the new authorization window.
How Can I Prepare?
Begin by confirming whether your test date falls before or after July 1, 2027. Study materials should match the content outline and scoring system that apply to your appointment.
For the current exam, complete practice built around developing case studies rather than relying entirely on isolated multiple-choice questions.
NCMHCE Study Checklist
- Review professional ethics, informed consent, confidentiality, and documentation.
- Practice biopsychosocial assessments and diagnostic interviews.
- Review mental status examination findings.
- Study risk assessment for suicide, homicide, abuse, and other emergencies.
- Review DSM-5-TR diagnostic criteria and differential diagnosis.
- Practice identifying co-occurring mental health and substance-use conditions.
- Develop measurable treatment goals and objectives.
- Match counseling interventions to client needs and clinical evidence.
- Review crisis intervention, de-escalation, referral, and level-of-care decisions.
- Study individual, group, couples, and family counseling principles.
- Review culturally responsive and developmentally appropriate counseling.
- Practice revising treatment when new clinical information appears.
- Complete full-length practice under the 225-minute limit.
- Review the explanation for every missed answer and every correct answer obtained through guessing.
Case-Study Strategy
- Read only the information currently available in the case.
- Do not assume facts that have not been provided.
- Identify immediate safety, ethical, and legal concerns first.
- Separate assessment actions from treatment interventions.
- Consider culture, identity, development, family systems, and client preferences.
- Choose the response appropriate for the current stage of counseling.
- Review every answer before moving to the next case-study section.
Clinical Decision Strategy
- Gather enough information before making a diagnosis or treatment decision.
- Use the least restrictive appropriate level of care.
- Prioritize client safety and stabilization during a crisis.
- Select interventions supported by the client’s diagnosis, needs, and preferences.
- Maintain professional boundaries and counselor competency.
- Consult, supervise, or refer when the client’s needs exceed the counselor’s role.
- Document significant clinical decisions accurately.
NCMHCE Study Resources
Top Study Guide:
Best Online Course:
High-Quality Flashcards:
Free Practice Resources:
NCMHCE®, NBCC®, National Clinical Mental Health Counseling Examination®, and National Board for Certified Counselors® are marks associated with the National Board for Certified Counselors, Inc. NBCC, CCE, and Pearson VUE are not involved with or affiliated with Mometrix Media LLC or StudyGuideZone.com, nor do they endorse or sponsor products or services offered by Mometrix Media LLC or StudyGuideZone.com.